
Our 4-Pillar Approach
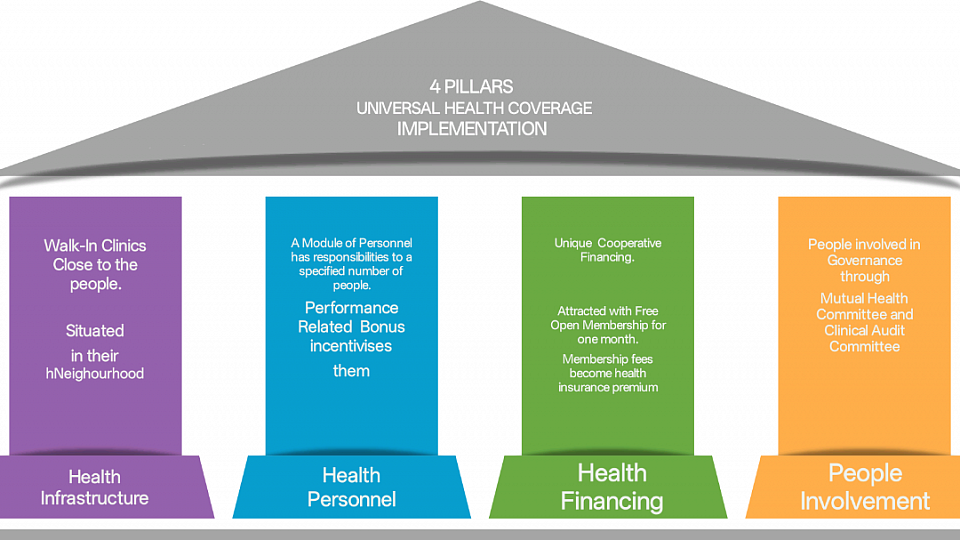
The 4 PILLARS
Implementing Universal Health Coverage In Nigeria
Pillar 1: AI Health Infrastructure within Neighbourhoods
Pillar 2: Dedicated Modules of Community Health Personnel
Pillar 3: Membership Fee As Health Financing, Health Insurance Premium
Pillar 4: Community People Involvement
Pillar 1: Primary Healthcare Infrastructure:
These are Open Access, Walk-In Mutual Clinics in peoples' neighbourhoods across the state. The Clinics will be AI enabled and equipped with essential medicines and essential diagnostic point of contact kits. The Clinics will publish daily working hours. The Clinics will operate with a protocol of referral to secondary care.
Pillar 2: Modules of hierarchical community health personnel
A dedicated Module of Personnel consists of 200 Key Workers recruited and trained to respond to contacts from the people about their health needs. The 200 Community Key Workers will be Task Sharing and Task Shifting with 6 qualified nurses using approved Clinical protocols supervised by a registered medical practitioner. The referral protocol uniquely includes public and private health institutions in the referral system.
Pillar 3: Health Financing and Health Insurance
Residents of the local neighbourhoods will have open access to the Walk-In Mutual Clinics. They will be enrolled as members of Mutual Health Associations. The membership fees of the MHA will be used as health insurance premium for the members.
Pillar 4: People Involvement
Local people will be recruited into Mutual Health Association Committees to manage the Walk-In Clinics by organising membership of the Mutual Health Association, MHA. The committees will carry out membership drives.
These 4 pillars combine Community Governed Primary Healthcare and Community Governed Health Insurance into an innovative Hybrid Model to deliver AI assisted Universal Health Coverage in Ekiti State, Nigeria
1. Background and Rationale
Nigeria has committed to Universal Health Coverage (UHC), yet insurance enrollment remains limited and out-of-pocket health expenditure remains high. Primary healthcare delivery is fragmented, and communities are often treated as service recipients rather than structural participants in financing and governance.
Healthcare Access Covenant Foundation (HAC) was established to translate UHC from policy aspiration into community-level implementation in which the people are at the core of management health insurance enrollment and governance of the system.
Our model aligns with the mandate of the National Health Insurance Authority of the federal government of Nigeria and global UHC principles advanced by the World Health Organization that primary health care is better achieved with involvement of the local people.
By its characteristics, Ekiti State provides a viable reform environment for piloting a scalable, cooperative-based primary healthcare system that integrates pre-paid financing of membership fees as insurance premium for primary health care services and accountable community governance.
2. Problem Statement
In Ekiti State, like the rest of Nigeria, the key challenges include:
* Low enrollment in structured health insurance mechanisms
* High out-of-pocket primary care expenditure
* Limited integration of private providers into insurance networks
* Weak community participation in health financing governance
* Vulnerable populations excluded from prepaid systems
Without structured enrollment and local ownership, progress toward UHC remains virtually impossible.
3. Project Goal
To establish a cooperative-based, community-governed primary healthcare network of clinics in Ekiti State, called Mutual Health Association Clinics. These integrate insurance financing, structured service delivery, and measurable accountability systems using the 4-Pillar approach.
4. Project Objectives (36 Months)
4.1 To establish 3–5 Community Mutual Health Association (MHA) AI Clinics in selected Ekiti communities, in the first year and 22 Clinics in the second year.
4.2 To Enroll 200,000 individuals for AI enabled primary healthcare delivery paid for by membership fees of the MHA as insurance premium.
4.3 To Provide targeted contribution subsidies to 5-10% of the registered membership identified through a validated means-testing protocol as vulnerable people.
4.4 Demonstrate measurable improvement in financial protection and primary care utilization.
4.5 To demonstrate sustainability of our health service-health insurance hybrid approach,
4.6 To publish outcomes demonstrating a scalable implementation framework for expansion within Southwestern Nigeria.
5. Intervention Model
RuralMind AI Clinics
Neighborhood-based clinics owned and governed cooperatively by members of the community.
Services include:
Preventive annual health assessments for all members
Free primary care consultations for all members
Essential medicines within approved protocols
Coordinated referrals for secondary health care, both public and private
Community-based follow-up after hospital discharge
6. Membership Structure
Open Membership free for one month
Insured Membership:
Open Members who pay their membership fees will become Insured Members to receive free service for one year.
Subsidy Framework
A community-validated, means-tested vulnerability assessment tool will be used to identify individuals who are VULNERABLE and eligible for sponsored membership contributions.
7. Expected Outcomes
By the end of Year 3:
*100% awareness of the benefits of pre-paid fees, health insurance, to gain quality health care.
*Increased insurance participation within target communities
*More than 10% of the population of Ekiti of 3.5 million people are enrolled in structured primary healthcare through membership of neighourhood MHAs
*Reduced risk of catastrophic out-of-pocket primary care expenditure
*Improved utilization of preventive and ambulatory services
*Community-elected governance structures actively overseeing clinical and ethical performance of primary health services.
*Contributing to Sustainable Development Goal 3 of the United Nations.
9. Monitoring & Evaluation
HAC will implement a structured Monitoring and Evaluation framework tracking:
Enrollment and retention rates of each Mutual Health Association
Service utilization indicators of the people, including the vulnerable people
Financial performance metrics
Member satisfaction
Comparative analysis with non-participating communities (where feasible)
Independent financial review and periodic impact reporting will be conducted.
10. Governance & Institutional Capacity
HAC operates under:
A Board of Trustees
Clinical Audit Committee
Community-elected members of Mutual Health Associations committees
Independent financial oversight mechanisms
Regular audit of Conflict-of-interest and financial disclosure policies in place
11. Funding Request
HAC seeks an investment of USD 1.2 – 1.8 million over 36 months to support:
Establishment of 40-50 Mutual Health Association neighbourhood RuralMind Clinics
Training and deployment of 2 Modules of health personnel each consisting of 100 CHW, 3 registered nurses, RN and 1 medical consultant.
Digital enrollment and health records systems
Initial staffing and operational support
Vulnerable household subsidy pool
Monitoring, evaluation, and independent assessment
Detailed budget breakdown and implementation timeline are available upon request.
12. Conclusion
Healthcare Access Covenant Foundation is building a structured, cooperative, community-owned primary healthcare model designed to advance Universal Health Coverage sustainably and at scale. This is not a health mission but a health system designed to be sustained by people involvement. It is health of the people, by the people, for the people.
This initiative represents an opportunity to move from policy commitment to measurable implementation within a replicable Nigerian context.
